Healthy Habitat
What has been a critical point of my interest, and a further point for dissection, is that we are living in the result of industrialization and urbanization as expressed by the current state of health in our country. Though we continuously talk about behavior change of the individual in the medical setting, there are contributing, almost invisible, factors that may constrain the individual in their decisions towards achieving better health. Our system surrounds episodic care, but health and wellbeing lives outside of physical medical spaces, on a spectrum of time and biological factors, and can be significantly influenced by the built environment in which we make decisions. This unequally impacts certain people over others, and I look forward to investigating this in Jonestown. For example, in focusing on issues relating to obesity, a third of adults are obese because only 1/5 of adults get enough physical activity. Many communities do not have access to safe sidewalks, recreation areas, or even fully stocked grocery stores. There are several other health considerations that perpetuate risk factors for chronic diseases, which feeds into Frumkin’s introductory statement of “we do not inherit the earth from our ancestors, we borrow it from our children”. Not only are we inherently changing the health potential of future generations because of our new genetic risk factors, but the environments we continue to build fail to consider health-oriented features. This also ties in to Nussbaum’s ‘capabilities approach’ to development, which centers around the question of ‘what are you able to do and be?' The environment around us shapes the potential of our lives and wellbeing, and should be fundamentally understood in the context of an individual's healthcare.
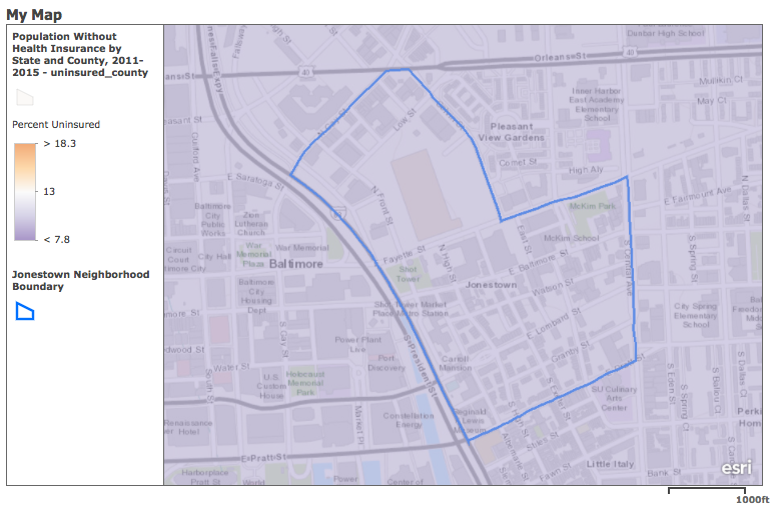
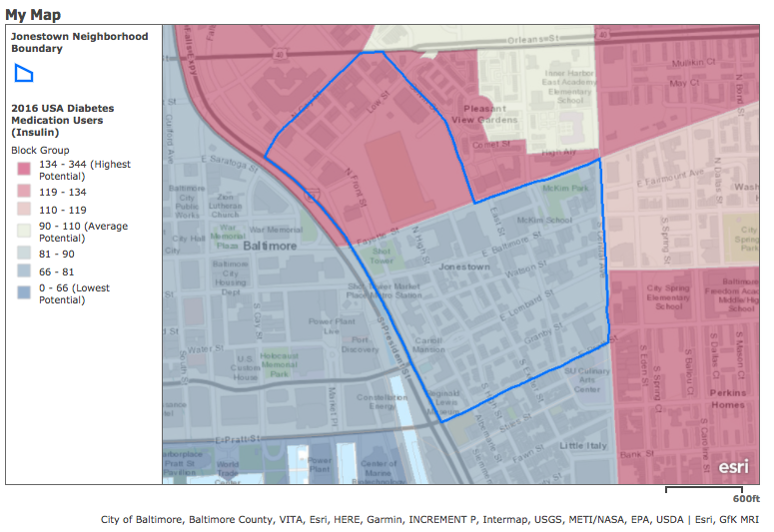
The maps of Jonestown display 1) health insurance access and 2) diabetes costs. What does this mean? Though Jonestown appears to have access to health insurance, in the North, there is a significantly higher incidence of diabetes. This leads to greater health expenditures and financial burdens on the individual, family, and community.
What are the underlying factors of the built environment that are contributing to this health outcome and disparity?
Healthy People
Baltimore has a lower life expectancy than both the US average, and the state of Maryland’s average. Concurrently, it ranks higher in the following; prevalence of alcohol use, prevalence of diabetes, prevalence of hypertension, and prevalence of obesity. Therefore, Baltimore should not be categorized as a healthy city, or as a habitat in which physical, social, and mental wellbeing are encouraged. Access to education, employment, healthy foods, etc. depends on the environment you are in, and therefore the promotion of good urban planning is critical for the wellbeing of it’s residents. 1.4 million people are added to urban areas each week, and it is important to have more than businesses, jobs, and GDP in mind for city development. For example, New York City now was a longer life expectancy than the average American. Initiatives to create a healthier urban population drive success, as seen with: bans on trans fats, criminalization of gun possession, making streets safer for bikers and pedestrians, expanding parks and recreational spaces, and reducing smoking. This is an example of a human development approach to improving cities.
Cohesive Communities
Cohesive communities are defined by a sense of belonging and socialization where there is trust, informal networks, access to formal networks, political involvement/representation, and equality in civil engagement. When communities feel more in control of their capacity, communal and individual resilience forms, which impacts mental health and wellbeing. In order to have capable, cohesive communities, there must be similar access to life opportunities, equal rights and responsibilities, and trust in each other and local institutions. Several successful programs have encouraged cohesion, such as increasing the community’s political voice, establishing interfaith coexistence through events, developing and maintaining community centers, and establishing partnerships and systemic collaboration to overcome barriers. However, limited economic opportunities, physical segregation of people from different backgrounds, and crime are negative predictors of cohesion and resilience. Identifying root causes of economic or social barriers is essential to eliminate stress, isolation, or discontent. Those with numerous needs and limited abilities are at higher risk, and networks of support at the local, state, and federal level should trickle down to support individuals. These deeply entrenched factors highly impact the Baltimore community, and may have obstructed cohesion within communities.
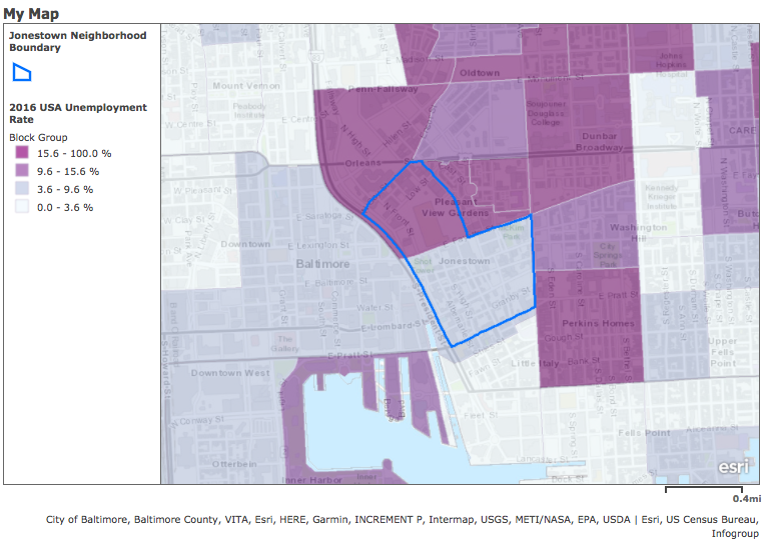
In the map below, we once again see the division between the north and south of Jonestown. The North has the highest unemplyment rate, which has significant implications around cohesiveness. There may be a lack of established partnerships or systemic collaboration to overcome barriers to work, such as transportations, health, childcare, debt management, or housing. These factors are significant in understanding capabilities, resilience, and health outcomes.
Engaged Citizens
Empowered, inclusive communities that are in charge of problem solving and advocating for the health and wellbeing of their neighborhoods is the goal for engaged citizenship. As cities and the individuals within them embrace technology, there are new opportunities to connect, consume, and lead. Though digitization may isolate and consumerize interactions, there is more importantly the embodiment of a citizen-centered approach where institutions are able to hear from people who previously felt voiceless. Anyone now has the opportunity to be engaged, and to weigh in through a more reciprocal process through social media, citizen engagement apps, etc. This type of broad participation strengthens democracy and governance at the local level, and can lead to cooperative, sustained change.
Shared Prosperity
Though world continues to increase wealth and spending power through a capitalistic economic and social structure, most people cannot share in the wealth or its benefits. The middle class in the US, as defined by the median, is smaller than any other country. Wealth inequality persists, an issue that is more concentrated in cities. Developing strong business ecosystems through building business-clusters, encouraging socially responsible investing, and harnessing broad-based ownership models could alleviate the gap in wealth. At the current state of technological development, further advancement could mean greater inequality between those who have these products/services and those who do not. It also has the potential to disrupt labor markets by pushing unskilled laborers to unemployment. However, technology could also increase possible safe jobs and opportunities in the globalizing world. In order to focus on the gains in opportunity and prosperity enabled by technology, there should be a focus on:
- Basic services and infrastructure
- Education and skills to guarantee access, quality, and equity.
- Economic inclusion through small business and financial assets ownership
- Fair wages/compensation
- Social protection through distributed fiscal advances
In Baltimore, the Urban Health Institute’s Henrietta Lacks Memorial Community Award winning organization Turnaround Tuesday is working on the ground level to build skillsets of those who are currently, or at risk for, joblessness. This grassroots dedication to welcome all people, provide training and support, and channel strong employer partnerships in the community like Johns Hopkins has a successful, inclusive strategy to address a core issue for the city of Baltimore. Uplifting community members in this way is a lesson in how a city can share prosperity, and how the shared benefits of this prosperity impacts to the community. This is the stepping stone to achieving engaged citizens, cohesive communities, healthy people, and a healthy habitat.
Background Photo by Reginald Thomas II
Make a free website with Yola